Chronic myelogenous leukemia
| Chronic myelogenous leukemia | |
|---|---|
| Classification and external resources | |
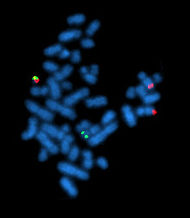 The Philadelphia chromosome as seen by metaphase FISH. |
|
| ICD-10 | C92.1 |
| ICD-9 | 205.1 |
| ICD-O: | M9875/3 |
| DiseasesDB | 2659 |
| MedlinePlus | 000570 |
| eMedicine | med/371 |
| MeSH | D015464 |
Chronic myelogenous (or myeloid) leukemia (CML), also known as chronic granulocytic leukemia (CGL), is a cancer of the white blood cells. It is a form of leukemia characterized by the increased and unregulated growth of predominantly myeloid cells in the bone marrow and the accumulation of these cells in the blood. CML is a clonal bone marrow stem cell disorder in which proliferation of mature granulocytes (neutrophils, eosinophils, and basophils) and their precursors is the main finding. It is a type of myeloproliferative disease associated with a characteristic chromosomal translocation called the Philadelphia chromosome. It is now treated with imatinib and other targeted therapies, which have dramatically improved survival.
Contents |
Signs and symptoms
Patients are often asymptomatic at diagnosis, presenting incidentally with an elevated white blood cell count on a routine laboratory test. In this setting, CML must be distinguished from a leukemoid reaction, which can have a similar appearance on a blood smear. Symptoms of CML may include: malaise, low-grade fever, gout, increased susceptibility to infections, anemia, and thrombocytopenia with easy bruising (although an increased platelet count (thrombocytosis) may also occur in CML). Splenomegaly may also be seen.[1][2]
Diagnosis

CML is often suspected on the basis on the complete blood count, which shows increased granulocytes of all types, typically including mature myeloid cells. Basophils and eosinophils are almost universally increased; this feature may help differentiate CML from a leukemoid reaction. A bone marrow biopsy is often performed as part of the evaluation for CML, but bone marrow morphology alone is insufficient to diagnose CML.[2][3]
Ultimately, CML is diagnosed by detecting the Philadelphia chromosome. This characteristic chromosomal abnormality can be detected by routine cytogenetics, by fluorescent in situ hybridization, or by PCR for the bcr-abl fusion gene.[2]
Controversy exists over so-called Ph-negative CML, or cases of suspected CML in which the Philadelphia chromosome cannot be detected. Many such patients in fact have complex chromosomal abnormalities which mask the (9;22) translocation, or have evidence of the translocation by FISH or RT-PCR in spite of normal routine karyotyping.[4] The small subset of patients without detectable molecular evidence of bcr-abl fusion may be better classified as having an undifferentiated myelodysplastic/myeloproliferative disorder, as their clinical course tends to be different from patients with CML.[5]
Pathophysiology
CML was the first malignancy to be linked to a clear genetic abnormality, the chromosomal translocation known as the Philadelphia chromosome. This chromosomal abnormality is so named because it was first discovered and described in 1960 by two scientists from Philadelphia, Pennsylvania, USA: Peter Nowell of the University of Pennsylvania and David Hungerford of the Fox Chase Cancer Center at Temple University. [6]
In this translocation, parts of two chromosomes (the 9th and 22nd by conventional karyotypic numbering) switch places. As a result, part of the BCR ("breakpoint cluster region") gene from chromosome 22 is fused with the ABL gene on chromosome 9. This abnormal "fusion" gene generates a protein of p210 or sometimes p185 weight (p is a weight measure of cellular proteins in kDa). Because abl carries a domain that can add phosphate groups to tyrosine residues (a tyrosine kinase), the bcr-abl fusion gene product is also a tyrosine kinase.[1][3]
The fused BCR-ABL protein interacts with the interleukin 3beta(c) receptor subunit. The BCR-ABL transcript is continuously active and does not require activation by other cellular messaging proteins. In turn, BCR-ABL activates a cascade of proteins which control the cell cycle, speeding up cell division. Moreover, the BCR-ABL protein inhibits DNA repair, causing genomic instability and making the cell more susceptible to developing further genetic abnormalities. The action of the BCR-ABL protein is the pathophysiologic cause of chronic myelogenous leukemia. With improved understanding of the nature of the BCR-ABLprotein and its action as a tyrosine kinase, targeted therapies have been developed (the first of which was imatinib mesylate) which specifically inhibit the activity of the BCR-ABL protein. These tyrosine kinase inhibitors can induce complete remissions in CML, confirming the central importance of bcr-abl as the cause of CML.[3]
Classification
CML is often divided into three phases based on clinical characteristics and laboratory findings. In the absence of intervention, CML typically begins in the chronic phase, and over the course of several years progresses to an accelerated phase and ultimately to a blast crisis. Blast crisis is the terminal phase of CML and clinically behaves like an acute leukemia. One of the drivers of the progression from chronic phase through acceleration and blast crisis is the acquisition of new chromosomal abnormalities (in addition to the Philadelphia chromosome).[1] Some patients may already be in the accelerated phase or blast crisis by the time they are diagnosed.[2]
Chronic phase
Approximately 85% of patients with CML are in the chronic phase at the time of diagnosis. During this phase, patients are usually asymptomatic or have only mild symptoms of fatigue or abdominal fullness. The duration of chronic phase is variable and depends on how early the disease was diagnosed as well as the therapies used. Ultimately, in the absence of curative treatment, the disease progresses to an accelerated phase.[2]
Accelerated phase
Criteria for diagnosing transition into the accelerated phase are somewhat variable; the most widely used criteria are those put forward by investigators at M.D. Anderson Cancer Center,[7] by Sokal et al.,[8] and the World Health Organization.[5][9] The WHO criteria are perhaps most widely used, and define the accelerated phase by any of the following:
- 10–19% myeloblasts in the blood or bone marrow
- >20% basophils in the blood or bone marrow
- Platelet count <100,000, unrelated to therapy
- Platelet count >1,000,000, unresponsive to therapy
- Cytogenetic evolution with new abnormalities in addition to the Philadelphia chromosome
- Increasing splenomegaly or white blood cell count, unresponsive to therapy
The patient is considered to be in the accelerated phase if any of the above are present. The accelerated phase is significant because it signals that the disease is progressing and transformation to blast crisis is imminent.[5]
Blast crisis
Blast crisis is the final phase in the evolution of CML, and behaves like an acute leukemia, with rapid progression and short survival.[2] Blast crisis is diagnosed if any of the following are present in a patient with CML:[10]
- >20% myeloblasts or lymphoblasts in the blood or bone marrow
- Large clusters of blasts in the bone marrow on biopsy
- Development of a chloroma (solid focus of leukemia outside the bone marrow)
Treatment
Chronic phase
Chronic phase CML is treated with inhibitors of tyrosine kinase, the first of which was imatinib mesylate (marketed as Gleevec or Glivec; previously known as STI-571). In the past, antimetabolites (e.g. cytarabine, hydroxyurea), alkylating agents, interferon alfa 2b, and steroids were used, but these drugs have been replaced by imatinib. Imatinib was approved by the United States FDA in 2001 and specifically targets BCR/abl, the constitutively activated tyrosine kinase fusion protein caused by the Philadelphia chromosome translocation. It is better tolerated and more effective than previous therapies. The IRIS study is an international study that compared interferon/cytarabine combination with imatinib. Long term follow up demonstrating the superiority of imatinib regimens is clear cut. However, the data of this study which allowed cross-over to Glivec has never been presented in an intent to treat analysis. It is not yet known whether Glivec treatment following cytarabine/interferon is better than Glivec alone in the long term. Bone marrow transplantation was also used as initial treatment for CML in younger patients before the advent of imatinib and; while it can often be curative, there was a high rate of transplant-related mortality. The transplant-related mortality rate as of 2010[update] is less than 5%. [3]
As described below, a number of newer drugs are being used to treat the minority of patients who develop imatinib resistance. Trials such as SPIRIT II are being carried out, to evaluate these newer drugs as 'upfront' therapy for patients with newly diagnosed chronic phase CML.
To overcome imatinib resistance and to increase responsiveness of TK inhibitors, two novel agents have been developed. The first, dasatinib, is a TK inhibitor that blocks several oncogenic proteins and was approved by the US FDA in 2007 to treat CML patients who are either resistant to or intolerant of imatinib. Another TK inhibitor, nilotinib, has also been approved by the US FDA for the same indication. Nilotinib is designed to bind more tightly than imatinib to the Bcr-Abl abnormal fusion protein responsible for chronic myeloid leukemia. Dasatanib is being compared with Imatinib for first-line therapy in the SPIRIT II trial being undertaken in the United Kingdom. Study on the combination of alpha Interferon with Imatanib is currently recruiting in higher risk patients in chronic phase CML.
Dasatanib and nilotinib failed to overcome the imatinib resistance caused by the T315I mutation. All current treatments for this mutation are experimental. Recently Chemgenex released results of their open-label Phase 2/3 study (CGX-635-CML-202) which investigated the use of omacetaxine, administered subcutaneously in CML patients who had failed imatinib and who have the highly drug-resistant T315I kinase domain mutation.
Stem cell transplantation is an option for patients who developed T315I mutation.[11][12]
In 2005 favourable results of vaccination were reported with the BCR/abl p210 fusion protein in patients with stable disease, with GM-CSF as an adjuvant.[13]
Prognosis
In one analysis of several clinical studies, three different risk groups were identified based on a prognostic scoring system that includes several variables: age, spleen size, blast count, platelet count, eosinophil count and basophil count. In the lowest risk group, the median survival time was 98 months. In the middle group, the median was 65 months, and in the highest risk group, the median was about 42 months. Of all patients analyzed, the longest survival time was 117 months.[14] However, this study pre-dates the advent of treatments using targeted therapy. A follow-up on patients using imatinib published in the New England Journal of Medicine shows an overall survival rate of 89% after five years.[15]
Epidemiology
CML occurs in all age groups, but most commonly in the middle-aged and elderly. Its annual incidence is 1–2 per 100,000 people, and slightly more men than women are affected. CML represents about 15–20% of all cases of adult leukemia in Western populations.[1] The only well-described risk factor for CML is exposure to ionizing radiation; for example, increased rates of CML were seen in people exposed to the atomic bombings of Hiroshima and Nagasaki[16]
References
- ↑ 1.0 1.1 1.2 1.3 Faderl S, Talpaz M, Estrov Z, Kantarjian HM (1999). "Chronic myelogenous leukemia: biology and therapy". Annals of Internal Medicine 131 (3): 207–219. PMID 10428738.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 Tefferi A (2006). "Classification, diagnosis and management of myeloproliferative disorders in the JAK2V617F era". Hematology Am Soc Hematol Educ Program 2006: 240–245. doi:10.1182/asheducation-2006.1.240. PMID 17124067.
- ↑ 3.0 3.1 3.2 3.3 Hehlmann R, Hochhaus A, Baccarani M; European LeukemiaNet (2007). "Chronic myeloid leukaemia". Lancet 370 (9584): 342–50. doi:10.1016/S0140-6736(07)61165-9. PMID 17662883.
- ↑ Savage DG; Szydlo RM; Goldman JM (1997). "Clinical features at diagnosis in 430 patients with chronic myeloid leukaemia seen at a referral centre over a 16-year period". Br J Haematol 96 (1): 111–116. doi:10.1046/j.1365-2141.1997.d01-1982.x. PMID 9012696.
- ↑ 5.0 5.1 5.2 Tefferi A, Thiele J, Orazi A, Kvasnicka HM, Barbui T, Hanson CA, Barosi G, Verstovsek S, Birgegard G, Mesa R, Reilly JT, Gisslinger H, Vannucchi AM, Cervantes F, Finazzi G, Hoffman R, Gilliland DG, Bloomfield CD, Vardiman JW (2007). "Proposals and rationale for revision of the World Health Organization diagnostic criteria for polycythemia vera, essential thrombocythemia, and primary myelofibrosis: recommendations from an ad hoc international expert pane". Blood 110 (4): 1092–1097. doi:10.1182/blood-2007-04-083501. PMID 17488875.
- ↑ Nowell PC (2007). "Discovery of the Philadelphia chromosome: a personal perspective". Journal of Clinical Investigation 117 (8): 2033–2035. doi:10.1172/JCI31771. PMID 17671636.
- ↑ Kantarjian H, Dixon D, Keating M, Talpaz M, Walters R, McCredie K, Freireich E (1988). "Characteristics of accelerated disease in chronic myelogenous leukemia". Cancer 61 (7): 1441–6. doi:10.1002/1097-0142(19880401)61:7<1441::AID-CNCR2820610727>3.0.CO;2-C. PMID 3162181.
- ↑ Sokal J, Baccarani M, Russo D, Tura S (1988). "Staging and prognosis in chronic myelogenous leukemia". Semin Hematol 25 (1): 49–61. PMID 3279515.
- ↑ Vardiman J, Harris N, Brunning R (2002). "The World Health Organization (WHO) classification of the myeloid neoplasms". Blood 100 (7): 2292–302. doi:10.1182/blood-2002-04-1199. PMID 12239137. http://www.bloodjournal.org/cgi/content/full/100/7/2292. Retrieved 2007-09-22.
- ↑ Karbasian Esfahani M, Morris EL, Dutcher JP, Wiernik PH (2006). "Blastic phase of chronic myelogenous leukemia". Current Treatment Options in Oncology 7 (3): 189–199. doi:10.1007/s11864-006-0012-y. PMID 16615875.
- ↑ Jabbour E, Cortes JE, Giles FJ, O'Brien S, Kantarjian HM (2007). "Current and emerging treatment options in chronic myeloid leukemia". Cancer 109 (11): 2171–2181. doi:10.1002/cncr.22661. PMID 17431887.
- ↑ Kimura S, Ashihara E, Maekawa T (2006). "New tyrosine kinase inhibitors in the treatment of chronic myeloid leukemia". Current Pharmaceutical Biotechnology 7 (5): 371–379. doi:10.2174/138920106778521532. PMID 17076652.
- ↑ Bocchia M, Gentili S, Abruzzese E, Fanelli A, Iuliano F, Tabilio A, Amabile M, Forconi F, Gozzetti A, Raspadori D, Amadori S, Lauria F (2005). "Effect of a p210 multipeptide vaccine associated with imatinib or interferon in patients with chronic myeloid leukaemia and persistent residual disease: a multicentre observational trial". Lancet 365 (9460): 657–62. doi:10.1016/S0140-6736(05)17945-8. PMID 15721470.
- ↑ Hasford J, Pfirrmann M, Hehlmann R, Allan NC, Baccarani M, Kluin-Nelemans JC, Alimena G, Steegmann JL, Ansari H (1998). "A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group". Journal of the National Cancer Institute 90 (11): 850–858. doi:10.1093/jnci/90.11.850. PMID 9625174.
- ↑ Druker BJ, Guilhot F, O'Brien SG et al. (2006). "Five-Year Follow-up of Patients Receiving Imatinib for Chronic Myeloid Leukemia". New England Journal of Medicine 355 (20): 2408–2417. doi:10.1056/NEJMoa062867. PMID 17151364. http://content.nejm.org/cgi/content/full/355/23/2408.
- ↑ Moloney WC (1987). "Radiogenic leukemia revisited". Blood 70 (4): 905–908. PMID 3477299.
External links
- Chronic Myeloid Leukemia at American Cancer Society
- CML information from The Leukemia & Lymphoma Society
- Merck Manual:Chronic Myelocytic Leukemia (CML)
|
|||||||||||||||||||||||||||||||||||||||||||||||